Researchers believe a 2-year-old boy who died last December in a village in Guinea, was the first casualty of West Africa’s ongoing Ebola outbreak.
Since then, Ebola has spread to the neighboring countries of Sierra Leone, Liberia and Nigeria. By September 8, the World Health Organization (WHO) estimated the virus had infected 4,290 people and killed 2,296 of them — figures that the organization earlier said might actually be “two to four times higher than that currently reported” in areas of high transmission. WHO warned that the epidemic could infect more than 20,000 people before it is contained.
Doctors Without Borders, or Médecins Sans Frontières (MSF) as it is known internationally, began its Ebola intervention in March 2014, and now runs five Ebola management centers in the affected countries.
FRONTLINE spoke to Estrella Lasry, a tropical medicine adviser at MSF, who has managed previous infectious disease outbreaks in Africa, about why this one is so deadly, the challenges facing MSF’s field workers, and their efforts to train more health workers.
Why has this particular Ebola outbreak become the worst on record?
One of the reasons is Ebola was not known in this part of Africa so it took longer to identify as the cause than it usually would have. You see now what’s happened in [the Democratic Republic of] Congo, immediately the samples were sent to test for Ebola. Ebola is a known disease in that area. But it took longer for people to consult and to identify this as a potential infectious disease [in West Africa].
And the other thing is that it very quickly spread to urban areas. It’s very difficult to control an outbreak of a disease as infectious as Ebola once it’s in an urban area, because you have to trace back all the contacts that infected people have had in the past 21 days. In rural settings, you have encounters with the same people repeatedly, whereas in urban settings, you have close physical contact with different people all the time. When you start getting into public transportation or medical facilities, it just amplifies quicker than it would in a rural area.
“This is the biggest outbreak that we’ve ever known, and it’s also been the longest in terms of duration.”Those are the two main reasons we know, and that we can identify. I’m sure there are other reasons that are inherent to the virus that we don’t know at this point.
And this is the Zaire strain of the Ebola virus, correct?
Yes. The other thing is it presented with symptoms a little different from usual, so a lot of gastroenterological symptoms like vomiting, diarrhea. Initially, it would not be identified as Ebola, so that’s why they changed the name from Ebola hemorrhagic fever to Ebola viral disease. That also contributed to a later identification and wider amplification of the disease.
Once it was identified in March, it has still continued spreading. It’s not just the late identification, it’s the lack of knowledge, the fear, the people not wanting to come to medical facilities, people not being prepared enough in medical facilities, lack of proper infection control, a very poor existing health system. It’s a combination of a lot of factors, and not one single cause.
On Aug. 25, the World Health Organization released figures saying more than 240 health workers had been infected with Ebola, and more than half of them had died. Can you talk about the issues with finding experienced health workers to help tackle this outbreak? How are they handling the heightened risks?
It’s very difficult to find experienced workers. A lot of the national staff in these countries were infected or died at the beginning of the outbreak, when they still didn’t have the experience in managing it, and they weren’t taking the appropriate precautions. And we’re talking about countries that already have very limited numbers of health staff.
For experienced medical staff that MSF is sending this is the biggest outbreak that we’ve ever known, and it’s also been the longest in terms of duration. A lot of the experienced people have gone to the field two, three, four times already. It’s exhausting as a field worker. We’re trying to keep the people that we send for a maximum of six weeks — and if we push it, maybe eight weeks. But that’s it, because the rhythm is unsustainable otherwise, and when you get really exhausted is when you start making mistakes, putting yourself or your colleagues in danger.
Because these outbreaks are rare and relatively contained and affect a very limited number of patients, usually there’s a very limited number of people with experience to respond to them. A lot of people have learned from this outbreak, so now we will have a much bigger pool for future outbreaks. It’s the duration and magnitude of the outbreak that is making it difficult in terms of finding the appropriate staff. We’re training staff, but you also require a lot of hands-on training and supervision to make sure. … There’s no place for mistakes.
How long does this kind of training take?
We’re doing two-day training right now in Brussels for MSF and non-MSF staff, including people from other NGOs. A lot of the training you learn by doing with people who are experienced and can tell you, “You can’t do this, you can’t do that.”
I’m tempted to say that’s the only way to truly learn it, so when you’re actually facing the risk and facing the extent of danger, you will do things exactly by the book.
The attention to detail that you put into training in New York or Brussels is going to be different to when you actually know that “Yes, I can get infected or I can get someone else infected. And there’s a 50 percent chance I’m not going to come out of it alive.” You put yourself in a very different situation.
Are people being trained right now?
Yes, we’re doing training every two weeks right now, in Brussels.
Can you talk about what the training entails? How do the health workers learn to protect themselves?
It’s very practical. It’s some theory in terms of: What is Ebola? What are the measures of infection control? What are the ways to protect yourself? What are the different aspects of an outbreak?
But there’s also a lot on how to set up an Ebola treatment center. There’s a part that covers what kind of patient care we can do, although there’s not a lot we can do once they’re in the isolation ward. There is training on water and sanitation within an Ebola center. There’s also a part on other aspects of the management of the outbreak, everything from trainings, to community education, health promotion, triage and safe burials.
A lot of it is what goes on within an isolation ward, how to set it up and how to move from low-risk areas to high-risk areas. The other part of it is about the rest of the intervention, including how to handle contact tracing and all that.
In terms of what we are using to protect ourselves, there are several things. If you understand how the disease is transmitted, then it’s easier to understand the measures of infection control. Every setting uses different measures of infection control.
If you’re going to do a rumor check or assess a suspected case in a village, what we do is we don’t talk to the patient straight in front of them. We’re at more or less arm’s-length, talking to the side of the patient because of the risk of contagion by droplet. And we have gloves if we’re going to touch the patient, otherwise no. At this point we’re not using masks, unless we know that a patient is coughing a lot or vomiting.
When we’re in the triage area in either Ebola facilities or non-Ebola facilities, it varies a little bit, but we’re wearing scrubs, rubber boots, gloves, a mask and goggles most of the time to protect all of the mucuses.
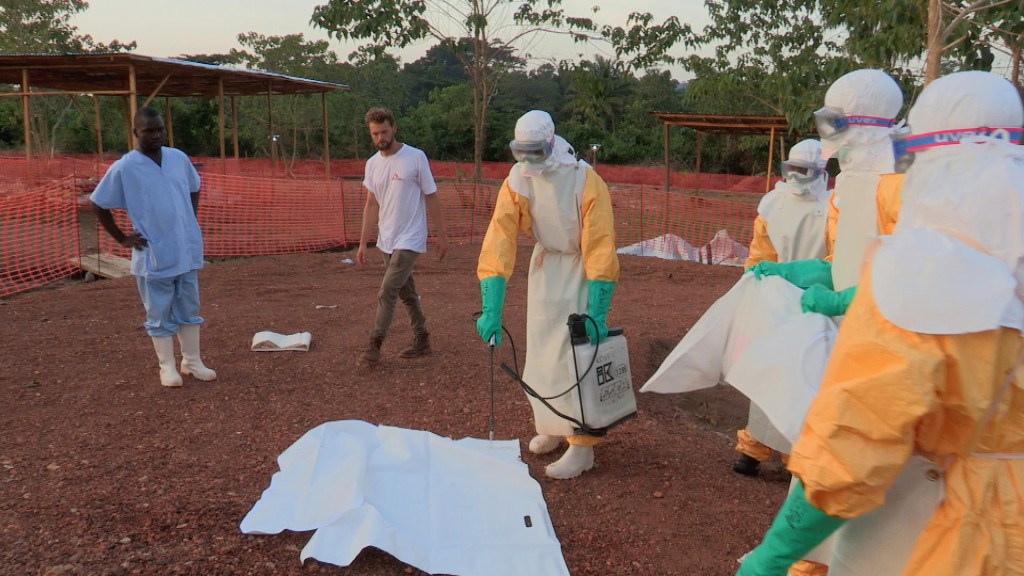
When we go into the [isolation] ward, we’re wearing full personal protective equipment, which means a Tyvek hazmat suit with a hood on top of it. The suit has a hood that comes with it, but we use another hood that covers the full head, the face, and has a mask, but we wear a mask underneath that as well. And then we have goggles on top of that, double or triple gloves, and boots, and an apron on top of that.
Another way to protect yourself is to go with someone, who — if you’re going to make a mistake or if you feel tired — will actually pull you out and say, “OK, let’s undress and we’ll go back at a later time.” You want to see more patients, and everything hurts but you stay in the ward for longer. What we’re trying to do is stay a maximum of 45 minutes in the ward, which makes it very difficult to see all of the patients.
For the burials, when we’re preparing the body we also wear a full protective suit, and once the body is in two body bags that have been sprayed we can actually carry it wearing scrubs, rubber gloves and boots.
The outbreak is being managed mainly by MSF Belgium, and then we have MSF Switzerland, Holland and Spain. The operational day-to-day management is mainly being done by Brussels. The Swiss also are working in Liberia. The Spanish are in Nigeria, in Congo and in Senegal. Eventually all of the sections are going to be involved in one way or another, whether it’s in directing the Ebola outbreak or basic health care.
Everyone’s kind of doing whatever they can. I’m going in October. I’m not sure where I’ll be going or what my role will be, but whatever’s needed at the time.
A recent update from MSF talked about an Ebola management center in Monrovia reaching capacity within its first week. How long does it take MSF to establish such centers, from the moment of decision?
It depends on the size, it depends on the place, and it depends on the staff that we have available. It can go anywhere from three to four days to a week, two weeks. It also requires a lot of negotiations with authorities and people on the ground to make sure it gets accepted and it’s not going to be burned down or attacked by the population because of fear.
We’re very quick in emergency response. If we can use existing construction, then we avoid having to do all the tents, but the tents go up pretty quickly. In one or two days, you can have a tent hospital set up. So one part is the hardware, and the other part is staffing, and that’s where our main constraint has been.
We’re very quick in setting things up, but staffing it appropriately is not always as easy.
“It’s very tough for the families to see one of their family members die, and then have to call on these people who are going to arrive, put on an astronaut suit and go into their houses and manage the body of their family member.”What makes the bodies of patients who died from Ebola more contagious? How does it complicate the matter of burial?
The burials are very sensitive for many reasons.
The moment a person dies is when their viral load is considered to be extremely high and all secretions are extremely contagious. That’s one of the things we’ve tried to do, is have trained burial teams so that the burials are done in an appropriate way. You have to handle the body in full protective equipment, spray the body, put it in a body bag, spray the body bag, put it in another body bag, spray the other body bag, and then burn all of the contaminated materials — sheets, clothes, mattress, buckets if a patient has been vomiting.
When you can access a patient it’s challenging, but it’s doable. The problem is you can’t always access the deceased before the family has started the cleansing of the body. … It’s very tough for the families to see one of their family members die, and then have to call on these people who are going to arrive, put on an astronaut suit and go into their houses and manage the body of their family member. It’s one of the very challenging parts of any Ebola outbreak, not only this one.
There’s a lot of mistrust. Even if we’ve been trying to build trust with the community since the beginning, it’s understandable that they have a hard time. There’s only so much we can do for the patients anyway once they go into the isolation ward. We can’t promise that their family members are going to come out alive.
Despite the high rates of infection and the staggering death toll, the mortality rate for this outbreak of Ebola seems lower than the feared 90 percent. What factors influence how deadly the virus is? Or is it arbitrary?
What causes increased or decreased mortality in each of the different countries is very difficult to know, and part of it is that we don’t really know the numbers. These are the numbers we’re seeing, but we’re not sure what is really out there. We may just be seeing, not the tip of the iceberg, but a chunk of the iceberg, but there’s certainly a part that we’re not seeing.
We don’t really know what the number of deaths are, and if the differences in mortality is just what we’re seeing, or if the virus is actually behaving a little differently. … The Zaire strain has one of the highest mortalities, but it has varied from one outbreak to the next. … I highly doubt that the virus will behave differently in the different settings, but that there’s a different awareness and access to healthcare in each of these countries.
There is no cure for Ebola currently, but is there any connection between how fast an infected person gets care and their chances for survival?
… If it’s the symptoms that are going to kill you, then yes. If it’s the lack of response to the disease itself or organ failure that’s going to kill you, then there’s not much that’s going to change from reaching a health facility earlier.
But the sooner you reach a health facility, the sooner you’re going to be putting less people in danger. So from a public health perspective, it has a huge impact to be treated early. For the individual patient, it’s a more limited impact.
In addition to more health workers, what else is needed to combat the virus in West Africa?
An increase in health promotion, more burial teams, an increase in psychosocial support for the communities so that they will be less scared, and eventually there will be acceptance and we are able to go into villages where we’re not being allowed to go right now and we’re just hearing rumors of people dying. Basically, we need people on the ground who will go out and do the legwork for all parts of the intervention.
Of course, we need health staff to be rotating with the staff that’s already there working extremely long hours seven days a week. But we also need staff that has less medical training, but can go out and talk to the community. What we do sometimes is we use survivors to then go out and do health promotion in the communities. But there are a limited number of survivors, and an even smaller number of survivors who want to do this. A lot of people just want to forget about it, go back and re-establish their normal life as much as possible.
Money is great. All contributions are very welcome, but at the end of the day if that doesn’t translate to having more people on the ground to do the actual work it’s not being used to its fullest potential.
“A lot of people just want to forget about it, go back and re-establish their normal life as much as possible.”There’s a need for training in the neighboring countries. The borders are still extremely porous even with this — I don’t know what they’re calling it in English, but in French it’s cordon sanitaire — on the borders of Mali and Ivory Coast and other countries, but the people aren’t properly trained. Proper training is necessary for all those people.
[NOTE: The cordone sanitaire is a strict quarantine, a tactic that The New York Times noted hadn’t been used in over a century. Despite its implementation, Senegal reported its first case of Ebola on Aug. 29, seen in a student who fled from neighboring Guinea, one of the countries hardest hit in this outbreak.]
What are some of the most common myths and pieces of misinformation MSF health workers encounter?
… It was more at the beginning than now. People thought that we were stealing bodies to do experiments, or to get organs, or get blood for other needs.
It’s more lack of trust than misinformation. People just have a lot of fear. We’re not being accepted into the communities because of the fear that we’re the ones bringing the disease. There was a lot of that fear at the beginning, and there’s less of it now, but it’s still there.
This happens in a lot of outbreaks, as well: Everybody who’s related to the diseased is a potential vector of the disease, and everyone who works at treatment centers, at MSF. We’re all considered potential vectors.
People are fearful of us because we have a direct connection with the disease.
With so many resources dedicated toward fighting Ebola, and losing many health workers to the virus, what has been the impact on patients suffering from other diseases?
It’s huge. There are women dying in labor because people refuse to do c-sections. There are people not being treated for malaria, and it’s the rainy season right now so it’s peak malaria season. There’s a general lack of staff in health care facilities. There was a very weak health care system to start with, and now a lot of the staff are either working in Ebola centers or they’ve been affected by the disease, so it’s very difficult to manage everything else that’s not Ebola.
Content retrieved from: http://www.pbs.org/wgbh/frontline/article/msf-on-ebola-this-is-the-biggest-outbreak-weve-ever-known/.